Case 1 - AneuRx TM Stent Graft Repair of Abdominal Aortic Aneurysm
Preoperative Evaluation
MP is an 81 year old woman who had an history of an abdominal aortic aneurysm since 1992. At that time it had measured 3.3 cm by ultrasound, but on a more recent evaluation had enlarged to 6.5 cm.
The patient is generally in good health. She has a remote history of a myocardial infarction but currently has no chest pain or shortness of breath. She can ambulate over a mile without angina. The patient has no history of cerebrovascular disease, hypertension, or diabetes.
On physical examination, the blood pressure was 94/62 and heart rate was 60. The patient had normal carotid pulses without any bruits. Neurologic examination is normal. The heart exam revealed no murmurs. The chest was clear. The abdomen revealed prominent, nontender pulsations consistent with the patient's known abdominal aortic aneurysm. The femoral, popliteal, and pedal pulses were normal.
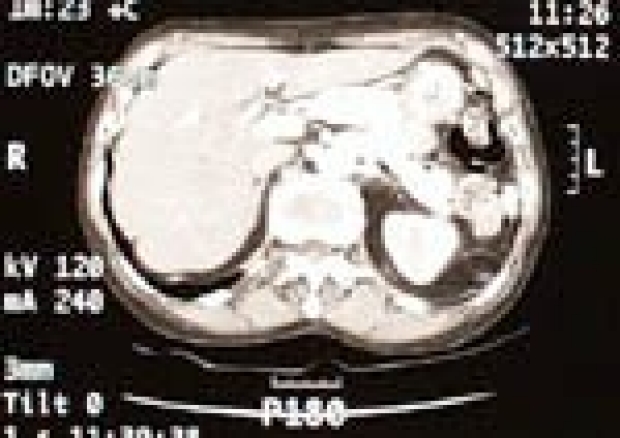
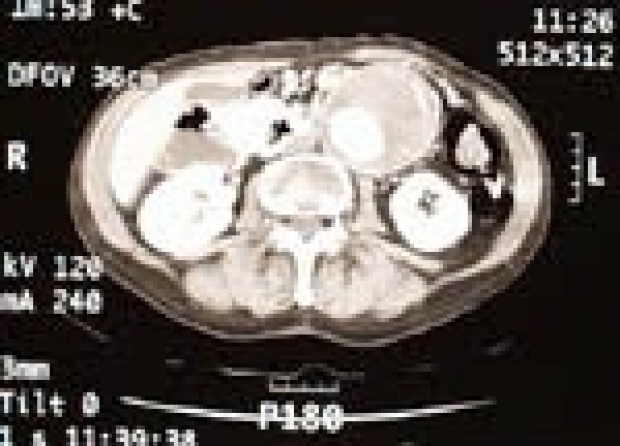
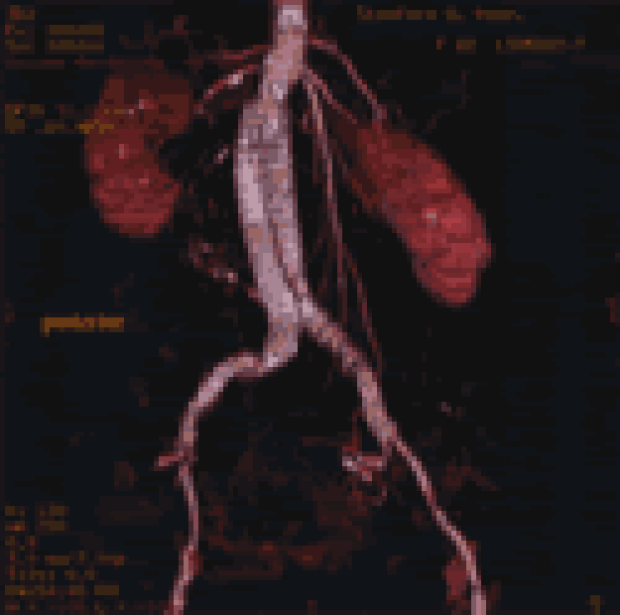
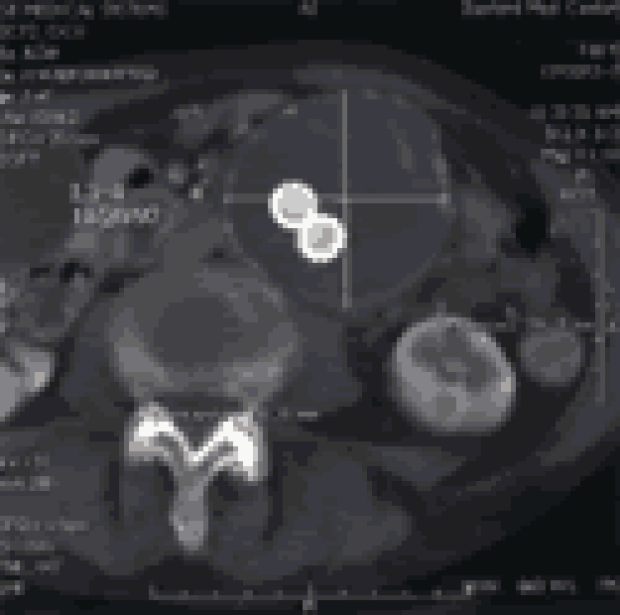
A spiral CT angiogram was performed with 3 mm cuts, which demonstrated an infrarenal aneurysm measuring 6.9 cm in greatest diameter:
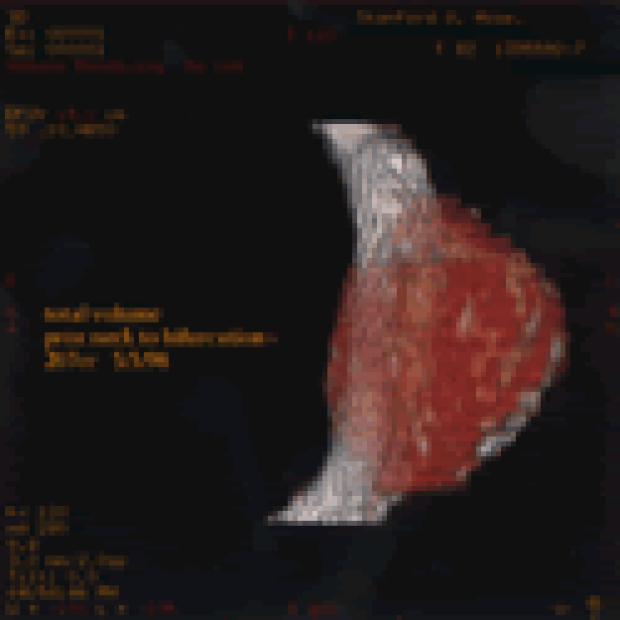
3-D reconstruction was performed with shaded surface displays and maximal intensity projections with center path length measurements:
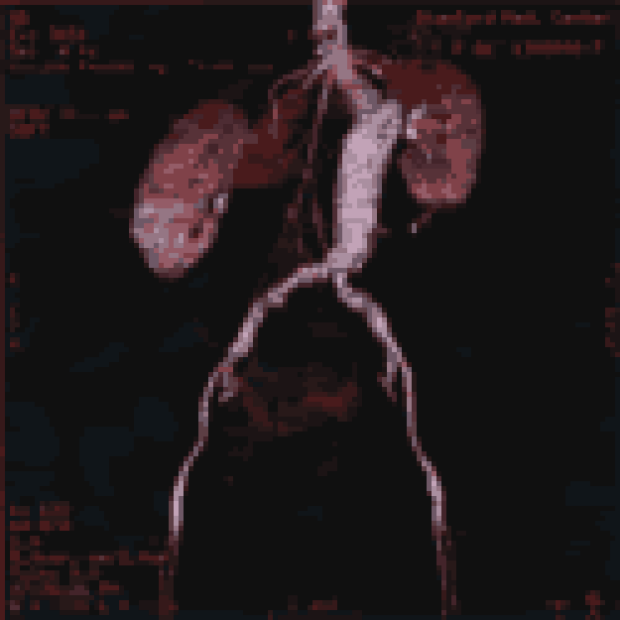
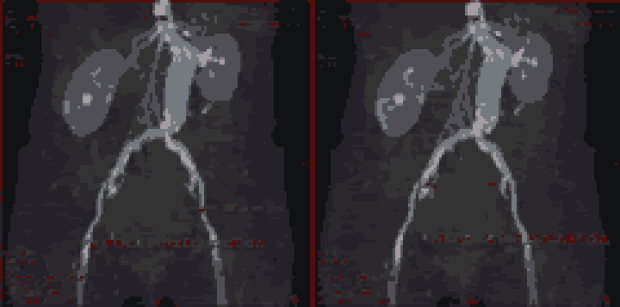
From these reconstructions, the dimensions of luminal diameter and length were obtained:
Diameters:
- Proximal neck: 16.9 x 16.4 mm
- Maximal transverse aortic: 69 x 66 mm
- Terminal aorta: 25 x 21 mm
- Right common iliac artery: 13.9 x 13.5 mm
- Left common iliac artery: 12.4 x 12.0 mm
Center path lengths:
- Proximal neck to start of aneurysm: 18 mm
- Proximal neck to distal right CIA: 228 mm
- Proximal neck to distal left CIA:204 mm
Given these dimensions, the patient's aneurysm was considered anatomically suitable for an endovascular repair using an AneuRxTM bifurcated stent graft device.
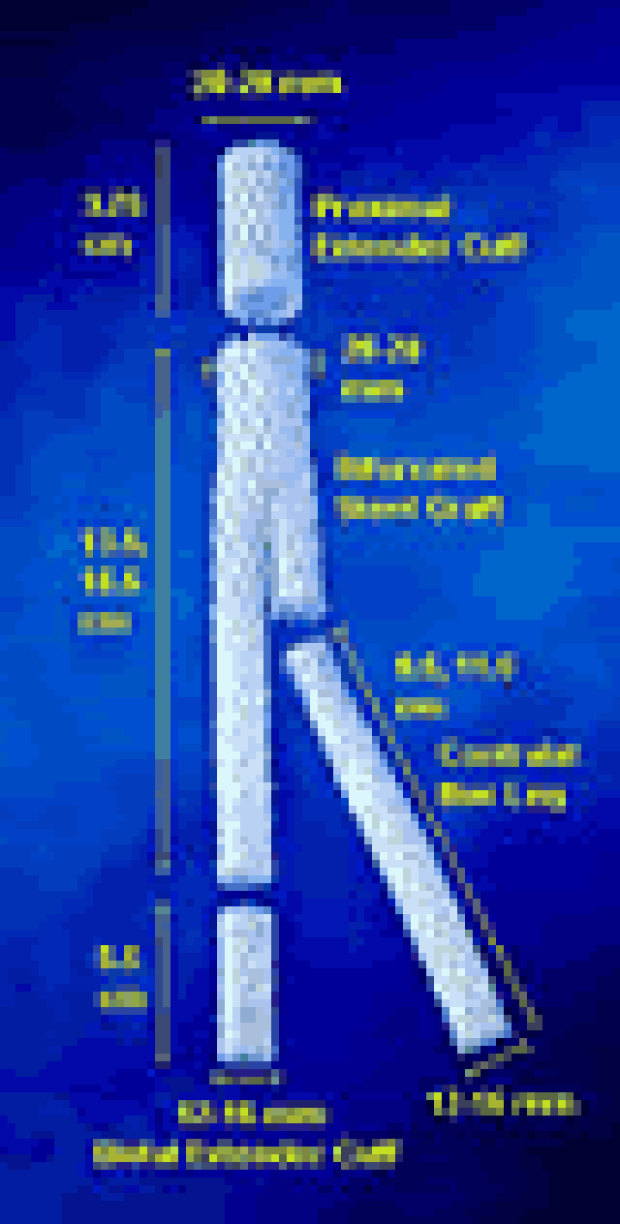
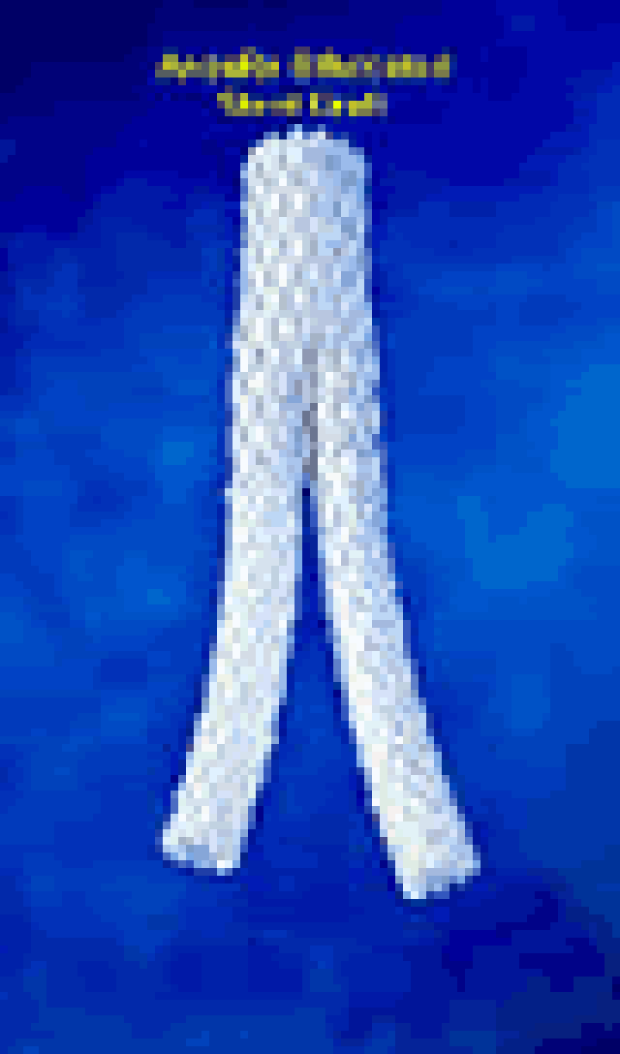
The AneuRx TM Stent Graft
The AneuRxTM stent graft is a modular, fully-covered, bifurcated aortic stent graft that is made with a thin Dacron graft externally supported by a Nitinol, self-expanding, stent. The primary module is deployed through a 22 F delivery sheath, and consists of the main endograft body with an ipsilateral limb. The contralateral limb is introduced through a 16 F sheath. Individual extender cuffs are available for placement at proximal or distal fixation sites:
Intraoperative Course

The procedure was performed in the operating room using an OEC 9600 mobile fluoroscopy unit and full motion digital processing capabilities.
After induction of general anesthesia, hemodynamic monitoring lines and a bladder drainage catheter are inserted. The patient is laid supine and preparation is routine for a standard abdominal aortic aneurysm repair. A Hemonetics cell-saver device is available but not routinely used.
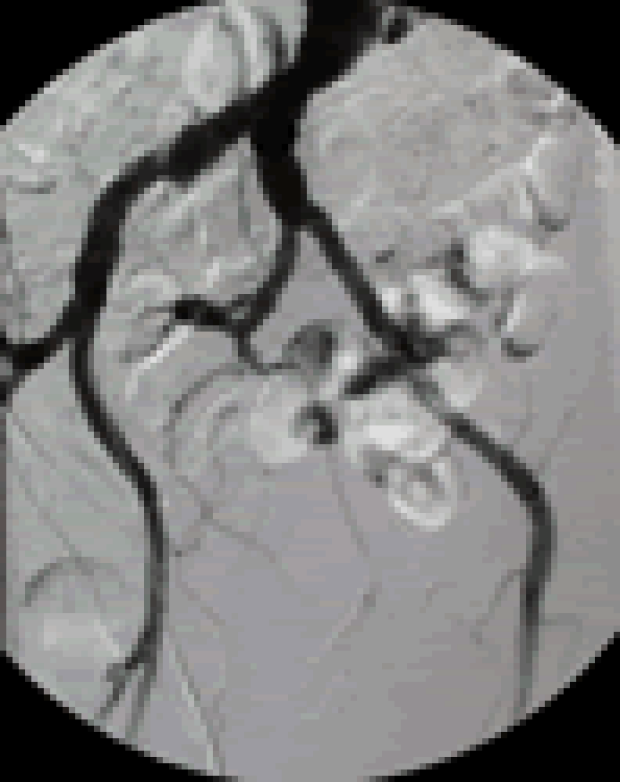
Through bilateral small oblique incisions made above the inguinal crease, a 2-3 cm segment of both common femoral arteries are exposed and controlled. The patient is systemically heparinized and the activated clotting time is maintained above 250 seconds by anesthesia. The access site for the primary module was on the right side. A 10 F sheath is introduced into the femoral artery through which a 5 F pig-tailed marker catheter is advanced to the level of L1-L2 vertebral body. An aortogram was performed for our initial roadmap.
This right femoral catheter was then exchanged for a 260 cm, 0.038-inch Amplatz SuperStiff guidewire. Given the previous dimensions measured by CT angiography with 3D reconstructions, a 22 mm (diameter of main body) x 13 mm (diameter of ipsilateral limb) x 16.5 cm (length of ipsilateral limb of the graft--see schematic) primary module and a 13 mm (diameter) x 11.5 mm (length) secondary module were chosen.
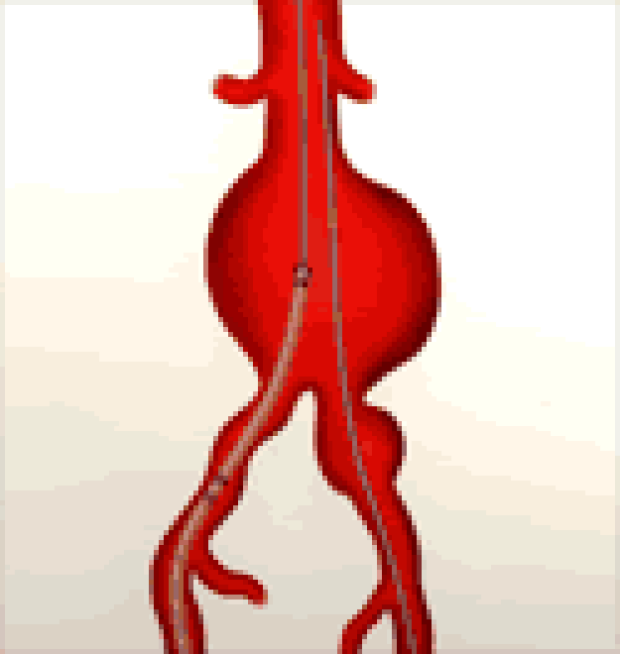
Initial access for the secondary limb through the left femoral artery using a .025 Bentsen wire and a 10 F sheath. A 22 F delivery sheath is carefully inserted through the right femoral artery over the SuperStiff guidewire. With the sheath properly positioned, the primary module is inserted and advanced to the level of the pararenal aorta based on previous roadmapping.
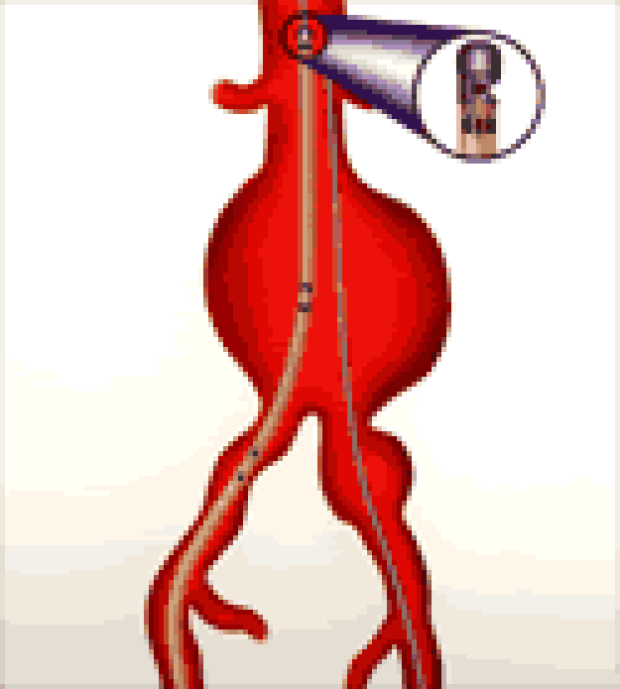
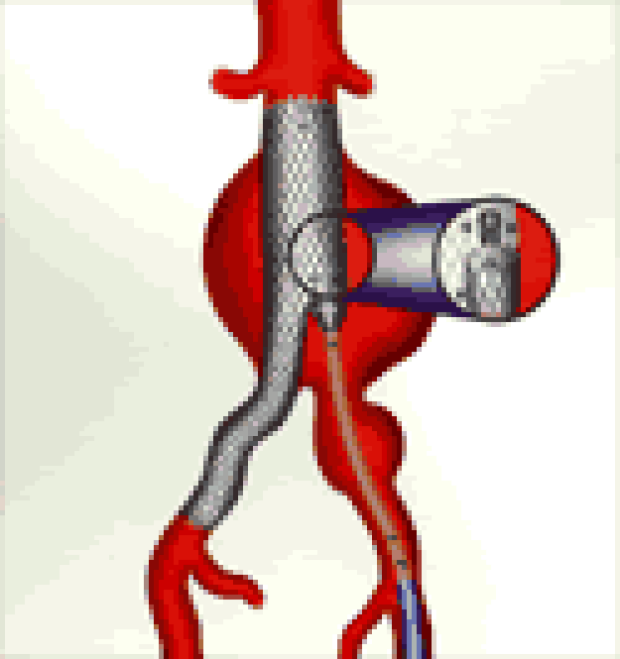
In these illustrations, the primary module is being advanced "bare," i.e. without a delivery sheath. The transverse orientation of the stent graft is set using the notch marking on the nose piece. The open end of the notch points to the side of the contralateral limb. The deployment begins at the suprarenal aorta by gradual, deliberate retraction of the graft cover using the deployment handle.
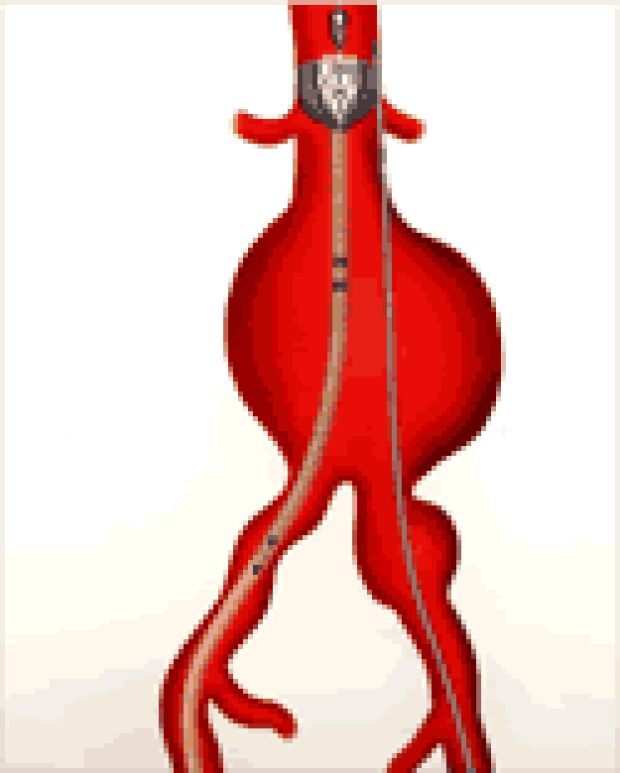
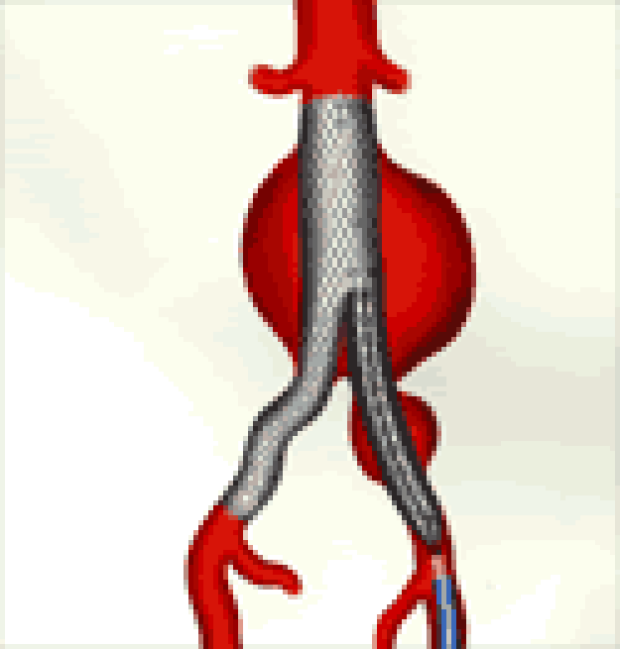
As deployment begins, repeat, small bolus, contrast aortography is performed around the pararenal aorta to precisely locate the origins of the renal arteries should any aortic displacement have occurred during insertion of the primary module. The partially deployed stent graft is moved caudally in millimeter increments until it is precisely positioned and the deployment completed. Through the previously placed left femoral sheath, the opening or the "gate" of the contralateral iliac limb is cannulated using standard guidewire techniques. This wire is exchanged for another .038 Amplatz SuperStiff guidewire. A 16 F delivery sheath is introduced and advanced into the iliac limb orifice.
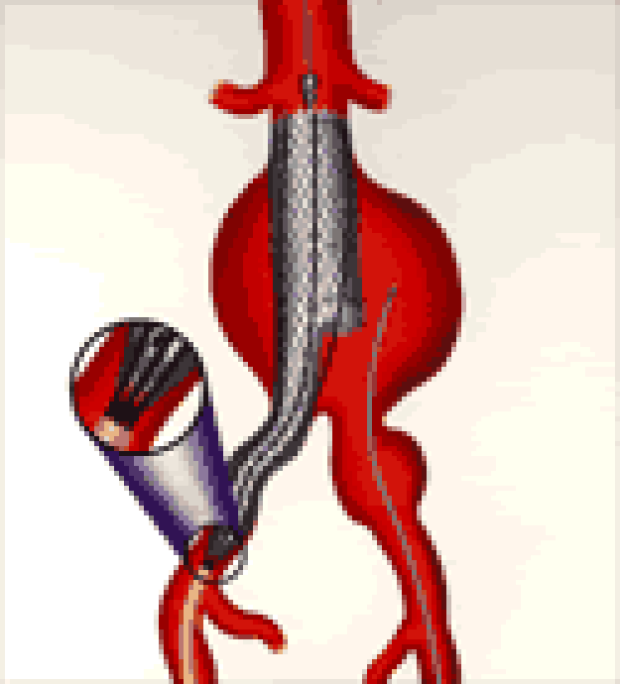
The secondary module containing the iliac stent graft is introduced through the sheath and carefully positioned within the gate using embedded radiopaque markers. Using the same deployment the graft cover is slowly retracted and deployment completed:
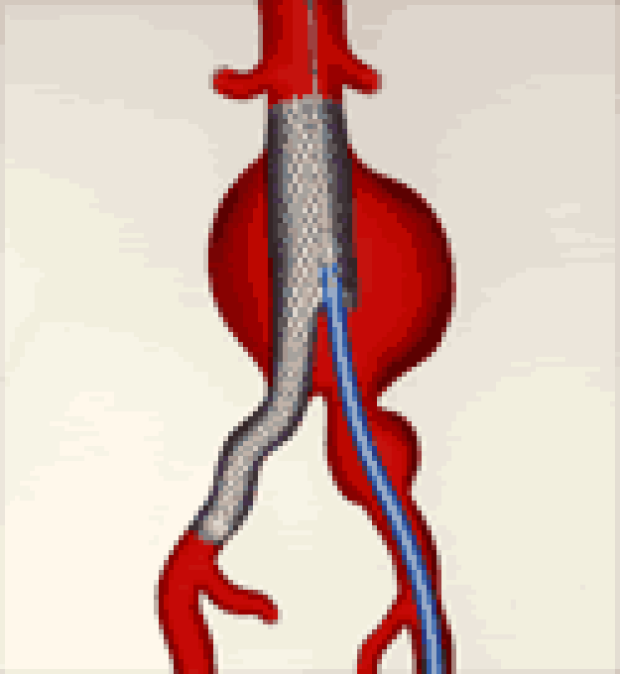
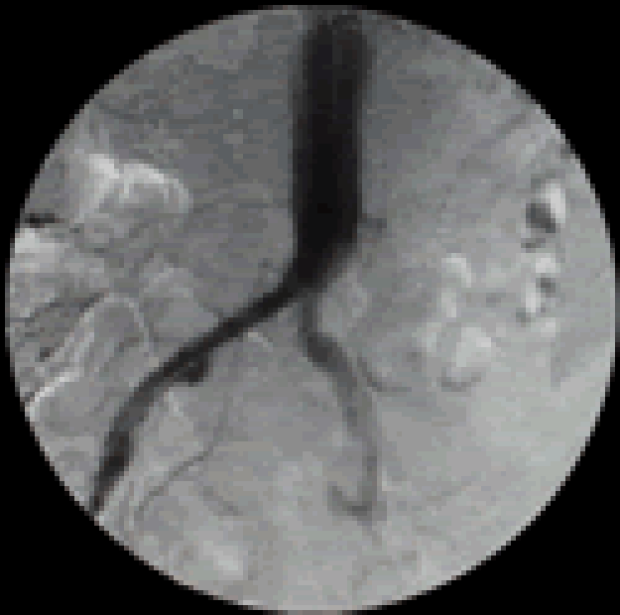
Following satisfactory deployment of both stent graft modules, a completion angiogram is performed to assess intraoperatively for proper positioning, patency of branch vessels, patency of the stent graft, and endoleaks:

The delivery sheaths were removed and the femoral arteriotomies were repaired primarily. The incisions were closed in a routine fashion, the patient was extubated, and moved to the Intensive Care Unit. Total estimated blood loss was 200 ml.
Postoperative Course

A postoperative baseline KUB is obtained in the ICU. This allows an assessment of any possible stent graft migration during followup evaluations.
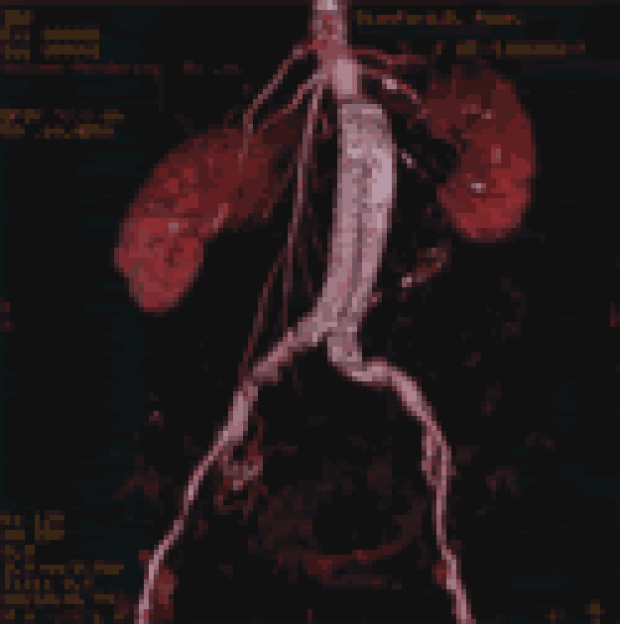
The patient's fluids were decreased and a regular diet resumed on the evening of the operation. She was transferred to the general care floor on postoperative day #1, remarked the noticeable absence of pulsations over her abdomen, and ambulated without difficulty. The patient did not receive any blood products, serum creatinine remained baseline, distal pulses were full and intact, and she was discharged on the morning of postoperative day #2. A postoperative CT angiogram and color-flow duplex ultrasound was obtained, which confirmed the correct placement of the stent graft with complete exclusion of the abdominal aortic aneurysm:

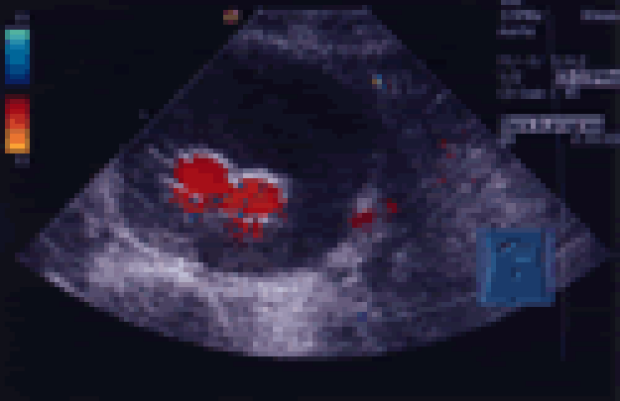

Follow-Up
At last follow-up, 6 months after her stent graft repair of the abdominal aortic aneurysm, the patient was doing well without any symptoms. Repeat duplex ultrasound imaging demostrated interval decrease in her aneurysm from a preoperative size of 7.4 cm to 6.6 cm, with a fully patent stent graft in good position, and no evidence of an endoleak.